A GLOBAL EPIDEMIC
SOME STATISTICS
Despite the fact that widespread concerns surrounding their use have abounded for many decades, benzodiazepines are still widely prescribed in most industrialized countries and diazepam is reputedly one of the most widely prescribed drugs of all time [8]. These concerns relate to their unfavorable side-effect profile, as well as their propensity for dependence [5]. Moreover, the clinical effectiveness of these drugs is a question of much debate and there is growing evidence that their chronic prescription is a matter of grave concern for health professionals, legislators and, most importantly, patients [1,8].
The benefits of benzodiazepine withdrawal have also been proven. For example, in a 3-year follow-up study, Rickels et al. [6] found that 73% of patients tapered off benzodiazepines were managing without anxiolytic medication 3 years after stopping these drugs compared with only 39% of patients who had reduced their use, but not stopped, the drugs and 14% of those that refused to participate in the original program. In elderly nursing home residents, measures of memory and cognitive function improved after they were tapered off benzodiazepines [7]. In one large community-based study in which 192 long-term benzodiazepine users were recruited in 25 GP practices, patients who successfully withdrew from benzodiazepines, with tapering, had improved performance on several psychomotor and cognitive tasks versus controls [2]. Economic benefits of benzodiazepine withdrawal also ensue since these drugs are prescribed frequently without clinical need or benefit, leading to a waste of resources [5,3].
- Arbanas, G.; Arbanas, D.; Dujam, K. Adverse effects of benzodiazepines in psychiatric outpatients. Psychiatr. Danub. 2009, 21, 103–107.
- Curran, H.; Collins, R.; Fletcher, S.; Kee, S.; Woods, B.; Iliffe, S. Older adults and withdrawal from benzodiazepine hypnotics in general practice: Effects on cognitive function, sleep, mood and quality of life. Psychol. Med. 2003, 33, 1223–1237.
- Cahir, C.; Fahey, T.; Teeling, M.; Teljeur, C.; Feely, J.; Bennett, K. Potentially inappropriate prescribing and cost outcomes for older people: A national population study. Br. J. Clin. Pharmacol. 2010, 69, 543–552.
- Donoghue, J.; Lader, M. Usage of benzodiazepines: A review. Int. J. Psychiatr. Clin. Prac. 2010, 14, 78–87.
- Lader, M.; Tylee, A.; Donoghue, J. Withdrawing benzodiazepines in primary care. CNS Drugs 2009, 23, 19–34.
- Rickels, K.; Case, W.G.; Schweizer, E.; Garcia-Espana, F.; Fridman, R. Long-term benzodiazepine users 3 years after participation in a discontinuation program. Am. J. Psychiatry 1991, 148, 757–761.
- Salzman, C.; Fisher, J.; Nobel, K.; Glassman, R.; Wolfson, A.; Kelley, M. Cognitive improvement following benzodiazepine discontinuation in elderly nursing home residents. Int. J. Geriatr. Psychiatry 1992, 7, 89–93.
- Spanemberg, L.; Nogueira, E.L.; Belem da Silva, C.T.; Dargel, A.A.; Menezes, F.S.; Neto, A.C. High prevalence and prescription of benzodiazepines for elderly: Data from psychiatric consultation to patients from an emergency room of a general hospital. Gen. Hosp. Psychiatry 2011, 33, 45–50.
General:
Despite the above and other expert warnings, the 2010 INCB Report (pg 32) shows that there was actually a general global increase in the previous decade.
Benzodiazepines are the most widely prescribed drugs in the world, used mainly as anxiolytics and hypnotics. —WHO 1996
United States:
A research paper published in 2016 by the American Journal of Public Health shows that, between 1996 and 2013, benzodiazepine prescriptions and overdose mortality have increased considerably in the US (See CNN report).
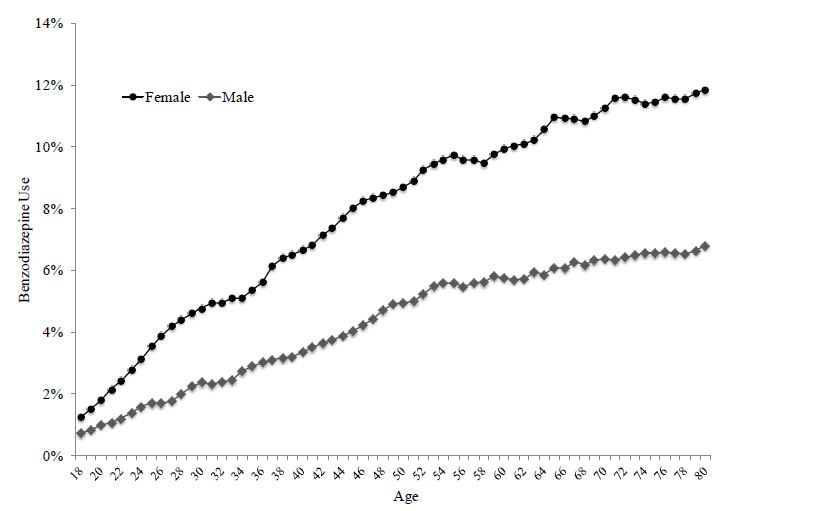
In 2008, approximately 5.2% of US adults aged 18 to 80 years used benzodiazepines. The percentage who used benzodiazepines increased with age from 2.6% (18-35 years) to 5.4% (36-50 years) to 7.4% (51-64 years) to 8.7% (65-80 years). Benzodiazepine use was nearly twice as prevalent in women as men. The proportion of benzodiazepine use that was long term increased with age from 14.7% (18-35 years) to 31.4% (65-80 years), while the proportion that received a benzodiazepine prescription from a psychiatrist decreased with age from 15.0% (18-35 years) to 5.7% (65-80 years). In all age groups, roughly one-quarter of individuals receiving benzodiazepine involved long-acting benzodiazepine use [2].
They [benzodiazepines] were involved in about 30% of prescription drug overdose deaths in 2013, second only to opioids, which were involved in 70% of overdose deaths, according to the Centers for Disease Control and Prevention [4]. The overdose death rate related to benzodiazepines more than quadrupled between 1999 and 2010, from 0.58 per 100,000 adults to 3.07 per 100,000 adults. The largest increase was among adults 18 to 64 years of age [3].
The percentage of adults in the United States who filled a benzodiazepine prescription per year [from 1996 to 2013] increased by about 30%, from 4.1% in 1996 to 5.6% in 2013. In addition, the amount of benzodiazepine medicine — whether Xanax, Valium, Ativan, Klonopin or other drugs in this class — in a prescription doubled over this time period. Anxiety was the most frequent reason these medications were given, accounting for 56% of prescriptions [3].
In 2006, a restrictive drug policy was introduced by one major insurer, for nursing home residents in the USA, excluding all benzodiazepines from reimbursement. Interestingly, this policy change led to an immediate reduction of circa 33% in their use in patients for whom no supplemental coverage for these medicines was available [1]. However, the same authors failed to find a clinical benefit for this reduction in use, possibly reflecting increased use of Z-drug hypnotics and/or the limited outcome measure that was studied (hip fracture). Replacing one drug dependency problem with another is not likely to provide a long-term solution to inappropriate prescribing practices.
In the 1980s, in New York State, stringent benzodiazepine prescribing restrictions produced higher prescribing of several more harmful barbiturate medications [7].
In the USA, Simon and Ludman [5] reported that 30% of 129 outpatients aged ≥60 with mixed diagnoses who received benzodiazepines continued its regular use for more than 2 months in primary care settings in western Washington State. In the HARP study, also in the USA (Harvard/Brown Anxiety Disorder Research Project), benzodiazepines were prescribed to 50% of all patients diagnosed with generalized anxiety disorder and up to one-third of those prescribed these drugs were taking them for as long as 12 years [6].
- Briesacher, B.A.; Soumerai, S.B.; Field, T.S.; Fouayzi, H.; Gurwitz, J.H. Medicare Part D’s exclusion of benzodiazepines and fracture risk in nursing homes. Arch. Intern. Med. 2010, 170, 693–698.
- JAMA Psychiatry. 2015 Feb;72(2):136-42. doi: 10.1001/jamapsychiatry.2014.1763.
- Marcus A. Bachhuber, Sean Hennessy, Chinazo O. Cunningham, and Joanna L. Starrels. Increasing Benzodiazepine Prescriptions and Overdose Mortality in the United States, 1996–2013. American Journal of Public Health: April 2016, Vol. 106, No. 4, pp. 686-688. doi: 10.2105/AJPH.2016.303061
- Prescription Opioid Overdose Data. (2016, December 16). Retrieved May 06, 2017, from https://www.cdc.gov/drugoverdose/data/overdose.html
- Simon, G.E.; Ludman, E.J. Outcome of new benzodiazepine prescriptions to older adults in primary care. Gen. Hosp. Psychiatry 2006, 28, 374–378.
- Vasile, R.G.; Bruce, S.E.; Goisman, R.M.; Pagano, M.; Keller, M.B. Results of a naturalistic longitudinal study of benzodiazepine and SSRI use in the treatment of generalized anxiety disorder and social phobia. Depress. Anxiety 2005, 22, 59–67
- Weintraub, M.; Singh, S.; Byrne, L.; Maharaj, K.; Guttmacher, L. Consequences of the 1989 New York State triplicate benzodiazepine prescription regulations. JAMA 1991, 266, 2392–2397.
France:
In the study, Gaining insight into benzodiazepine prescribing in General Practice in France: a data-based study, 12.5% of patients older than 18 were prescribed BZDs at least once during 2006 and the average (SD) was 2.6 (2.4) BZD prescriptions/patient/year [2].
In a French telephone survey of patients in 2001, the prevalence of benzodiazepine prescribing in a cross-section of community-dwelling adults was 7.5%, and factors associated with increased use of these drugs included advanced age, female gender and social disadvantage/unemployment [1]. Again, duration of usage commonly exceeds prescribing guidelines, with more than 75% of users being prescribed these drugs for more than 6 months [1].
- Lagnaoui, R.; Depont, F.; Fourrier, A.; Abouelfath, A.; Begaud, B.; Verdoux, H.; Moore, N. Patterns and correlates of benzodiazepine use in the French general population. Eur. J. Clin. Pharmacol. 2004, 60, 523–529
- Rosman, S., Marc, L. V., & Nathalie, P.-F. (2011). Gaining insight into benzodiazepine prescribing in General Practice in France: a data-based study. BMC Family Practice, 12, 28. http://doi.org/10.1186/1471-2296-12-28
Australia:
“In Australia, a decrease in benzodiazepine prescribing was achieved in the 1990’s following the issuing of revised prescribing guidelines and a public awareness campaign. However, since these campaigns ended, utilisation started to creep back up with a 21% increase in use from the years 2000–2006 observed in an elderly, socioeconomically disadvantaged population [1].”
- Smith, A.J.; Sketris, I.; Cooke, C.; Gardner, D.; Kisely, S.; Tett, S.E. A comparison of benzodiazepine and related drug use in Nova Scotia and Australia. Can. J. Psychiatry 2008, 53, 545–552.
Nova Scotia:
“The use of benzodiazepines in Nova Scotia was more than double that of Australia in 2000 (123 and 48 DDD/1000 beneficiaries per day, respectively) through 2003 (138 and 57 DDD/1000 beneficiaries per day, respectively). Eight different benzodiazepines made up 90% of the drug use in Nova Scotia by contrast to only 4 different benzodiazepines in Australia. [1]”
- Smith, A.J.; Sketris, I.; Cooke, C.; Gardner, D.; Kisely, S.; Tett, S.E. A comparison of benzodiazepine and related drug use in Nova Scotia and Australia. Can. J. Psychiatry 2008, 53, 545–552.
Norway:
In Norway, benzodiazepine use in the primary care setting was investigated with over 3,000 prescriptions written by GPs in a 2-month period being analyzed [1]. This indicated increasing dose with age, a higher proportion of prescribing to females, and a high percentage of repeat prescribing (82%), all of which point to a lack of compliance with National guidelines
- Straand, J.; Rokstad, K. General practitioners’ prescribing patterns of benzodiazepine hypnotics: Are elderly patients at particular risk for overprescribing? Scand. J. Prim. Health Care Suppl. 1997, 15, 16–21
Finland:
A population-based study in Finland found that one-third of home-based patients older than 75 years were using either benzodiazepines or related drugs chronically as sleeping aids or anxiolytics [1], while follow-up studies found that many of these users were taking these drugs on a long-term basis [2].
- Hartikainen, S.; Rahkonen, T.; Kautiainen, H.; Sulkava, R. Kuopio 75+ study: Does advanced age predict more common use of psychotropics among the elderly? Int. Clin. Psychopharmacol. 2003, 18, 163–167.
- Smith, A.J.; Sketris, I.; Cooke, C.; Gardner, D.; Kisely, S.; Tett, S.E. A comparison of benzodiazepine and related drug use in Nova Scotia and Australia. Can. J. Psychiatry 2008, 53, 545–552.
Ireland:
“In Ireland, a recent survey of potentially inappropriate prescribing in a population of over 70 year-olds included long-term (> 1 month) prescription of benzodiazepines in the elderly as a poor professional practice indicator [3]. Those authors identified high rates of long-term benzodiazepine use (13% in women and 5% in men) among this population as a major contributor to the overall statistic that one-third of the Irish population in this age-group are prescribed at least one potentially inappropriate drug on the basis of European best practice criteria. Only proton pump inhibitors and non-steroidal anti-inflammatories displayed a worse prevalence of inappropriate prescribing patterns.”
“In Ireland, a recent report commissioned by the government found that the number of prescriptions issued for benzodiazepines increased significantly in the period 2002–2008, despite an earlier report in 2002—the goal of which was to significantly reduce inappropriate use of benzodiazepines and attendant dependence on these drugs [1, 2]. Moreover, a recent ten-year follow-up study of community-dwelling older adults in which inappropriate psychotropic prescribing was assessed using Beer’s criteria, reported an overall prevalence rate of 6.5% for benzodiazepine use in those aged >65 years and a 27% inappropriate psychotropic prescribing rate for those over 75 years, the vast majority of which was accounted for by benzodiazepines [5]. In the institutional setting, chronic use of benzodiazepines is of particular concern in psychiatric hospitals and in residential nursing homes. One Irish study in which sequential admissions to a psychiatric hospital were monitored, indicated that 47% of patients were prescribed these drugs, usually without defined clinical need [4].”
- Bellerose, D.; Lyons, S.; Carew, A.; Walsh, S.; Long, J. Problem Benzodiazepine Use in Ireland: Treatment (2003 to 2008) and Deaths (1998 to 2007). Available online: http://www.drugsandalcohol.ie/14287/ (accessed on 7 May 2017).
- Benzodiazepines: Good Practice Guidelines for Clinicians. Available online: http://www.dohc.ie/ publications/benzodiazepines_good_practice_guidelines.html (accessed on 7 May 2017).
- Cahir, C.; Fahey, T.; Teeling, M.; Teljeur, C.; Feely, J.; Bennett, K. Potentially inappropriate prescribing and cost outcomes for older people: A national population study. Br. J. Clin. Pharmacol. 2010, 69, 543–552.
- Hallahan, B.; Murray, I.; McDonald, C. Benzodiazepine and hypnotic prescribing in an acute adult psychiatric in-patient unit. Psychiatr. Bull. 2009, 33, 12.
- O’Mhaolin, A.; Gallagher, D.; O’Connell, H.; Chin, A.; Bruce, I.; Hamilton, F.; Tehee, E.; Coen, R.; Coakley, D.; Walsh, B. Benzodiazepine use amongst community dwelling elderly: 10 years on. Int. J. Geriatr. Psychiatry 2010, 25, 650–651.
Denmark:
“In Denmark, it is illegal to write a benzodiazepine prescription exceeding four weeks, after which a full medical re-evaluation must assess their continued need [1].”
“BZD-use has been markedly reduced in the Danish population from 1997–2008; however, one in four people aged 75–85 years and almost one in three of patients over 85 years still use BZDs [2].”
- Committee on Safety of Medicines. Benzodiazepines, dependence and withdrawal symptoms. Curr. Probl. 1988, 21, 1–2.
- Holm, E., Fosbol, E., Pedersen, H., Jensen, T., Nielsen, M., Weeke, P., . . . Torp-Pedersen, C. (2012). Benzodiazepine use in Denmark 1997–2008. European Geriatric Medicine, 3(5), 299-303. doi:10.1016/j.eurger.2012.04.007
Netherlands:
In the Netherlands, circa 300 patients from 32 GP practices were recruited, half of whom were short-term benzodiazepines users and half long-term users. The long-term users were more likely to be older, to live alone, to be less well educated, to have a more serious mental health profile for which they had received prior treatment, to have attended hospital consultants more frequently, and to have a lower general health status [2,3].
A Dutch study, which looked at chronic users in three settings and applied both DSM-III-R and ICD-10 criteria for dependence, found that 40% of GP patients, 63% of psychiatric patients and 82% of those attending self-help groups were dependent on these medications [1]. In the same study drug type, age and educational attainment were also identified as predictors of long-term use.
- Mant, A.; Duncan-Jones, P.; Saltman, D.; Bridges-Webb, C.; Kehoe, L.; Lansbury, G.; Chancellor, A.H. Development of long term use of psychotropic drugs by general practice patients. BMJ 1988, 296, 251–254.
- .Zandstra, S.; van Rijswijk, E.; Rijnders, C.A.T.; van de Lisdonk, E.; Bor, J.; van Weel, C.; Zitman, F. Long-term benzodiazepine users in family practice: Differences from short-term users in mental health, coping behaviour and psychological characteristics. Fam. Pract. 2004, 21, 266–269
- Zandstra, S.M.; Furer, J.W.; van de Lisdonk, E.H.; Bor, J.H.; Zitman, F.G.; van Weel, C. Differences in health status between long-term and short-term benzodiazepine users. Br. J. Gen. Pract. 2002, 52, 805–808.
Hong Kong
In Hong Kong, a policy change including benzodiazepines as dangerous drugs, introduced in 1992, resulted in a 50% and a 10% reduction in the mean annual number of benzodiazepine prescriptions per person in the general and psychiatric populations, respectively, over the period 1991 to 1994 [1].
- Chung, K. Benzodiazepine prescribing trend after its inclusion as a dangerous drug under the Hong Kong dangerous drugs ordinance. Hong Kong Med. J. 1997, 3, 16–20.
Sweden:
“In Sweden, the prescription of long-acting benzodiazepines to a very elderly population of nursing home residents (mean age 85) was used as a poor prescribing indicator [1]. An inappropriate prescribing rate of 16% of patients was detected, with a number of prescribers per resident being positively correlated with poor prescribing performance.”
- Olsson, J.; Bergman, A.; Carlsten, A.; Oke, T.; Bernsten, C.; Schmidt, I.K.; Fastbom, J. Quality of drug prescribing in elderly people in nursing homes and special care units for dementia: A cross-sectional computerized pharmacy register analysis. Clin. Drug Investig. 2010, 30, 289–300.
UK:
“In a grouping of eight GP practices in Northern England, who were audited vs. their own good prescribing standards, only 31% met the acceptable standard of benzodiazepine prescription volume [1]”
In the UK, benzodiazepine prescribing is reported to be falling with the Z-drugs (zolpidem, zopiclone, and zaleplon) taking over, but the numbers being prescribed drugs for hypnosis are still very high and are not in alignment with guidelines issued by the UK National Institute of Clinical Excellence [2].
In the North of England, the vast majority of GPs surveyed viewed benzodiazepine use as problematic, despite its prevalence in their communities [3].
The following increases were reported in England from 2013 to 2014. Benzodiazepines: 7515 → 15,027, Z drugs (similar to benzodiazepines): 4723 → 11,054, Antidepressants: 14,558 → 28,393.
The 2014 Hospital Admissions Drug Poisoning Report, published by the NHS in England, has again shown that prescription drugs are causing people/society more harm than illegal drugs.
There are an estimated 1.5 million people suffering from doctor induced BZ drug dependency in England alone (with antidepressants now a major problem as well) − the number worldwide must be staggering. [4]
- Bateman, D.; Eccles, M.; Campbell, M.; Soutter, J.; Roberts, S.; Smith, J. Setting standards of prescribing performance in primary care: Use of a consensus group of general practitioners and application of standards to practices in the North of England. Br. J. Gen. Pract. 1996, 46, 20–25.
- National Institute for Health and Clinical Excellence. Clinical Guideline 113: Management of anxiety (panic disorder, with or without agoraphobia, and generalised anxiety disorder) in adults in primary, secondary and community care.
- Rogers, A.; Pilgrim, D.; Brennan, S.; Sulaiman, I.; Watson, G.; Chew-Graham, C. Prescribing benzodiazepines in general practice: A new view of an old problem. Health 2007, 11, 181–198.
- https://www.psychologytoday.com/us/blog/side-effects/201011/brain-damage-benzodiazepines-the-troubling-facts-risks-and-history-minor
European Countries:
In the ESEMeD study, psychotropic drug use across six European countries (Belgium, France, Italy, Germany, The Netherlands and Spain) was investigated. The authors found that anxiolytic medications were the most commonly used psychotropic drugs in these countries with an overall prevalence of 9.8% and concluded that these drugs were being used non-specifically for inappropriate disorders including depression [1]. Similarly, a four-country survey across France, Germany Italy and the UK found a particularly high rate of hypnotic prescribing in France (2.5%) with temazepam, flunitrazepam and nitrazepam accounting for over 40% of all hypnotic prescriptions [2].
- Alonso, J.; Angermeyer, M.; Bernert, S.; Bruffaerts, R.; Brugha, T.; Bryson, H.; Girolamo, G.; Graaf, R.; Demyttenaere, K.; Gasquet, I. Psychotropic drug utilization in europe: Results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr. Scand. 2004, 109, 55–64.
- Ohayon, M.M.; Lader, M.H. Use of psychotropic medication in the general population of France, Germany, Italy, and the United Kingdom. J. Clin. Psychiatry 2002, 63, 817–825.
Italy:
In Italy, trends in antidepressant and benzodiazepine use were tracked over a nine-year period and while antidepressant use tripled, benzodiazepine use was relatively stable [2]. However, two subsequent studies in Italy both documented a high prevalence of chronic use (mean of over 2 years) without increased dosage being used to counteract tolerance [3.4]. The prevalence rate of chronic benzodiazepine use for more than 1 year was also high in Italy Specifically it was found to be 90% in 177 patients aged 60 or older with anxiety disorders Balestrieri et al. [1]
- Balestrieri, M.; Marcon, G.; Samani, F.; Marini, M.; Sessa, E.; Gelatti, U.; Donato, F. Mental disorders associated with benzodiazepine use among older primary care attenders. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 308–315.
- Ciuna, A.; Andretta, M.; Corbari, L.; Levi, D.; Mirandola, M.; Sorio, A.; Barbui, C. Are we going to increase the use of antidepressants up to that of benzodiazepines? Eur. J. Clin. Pharmacol. 2004, 60, 629–634.
- Magrini, N.; Vaccheri, A.; Parma, E.; DíAlessandro, R.; Bottoni, A.; Occhionero, M.; Montanaro, N. Use of benzodiazepines in the Italian general population: Prevalence, pattern of use and risk factors for use. Eur. J. Clin. Pharmacol. 1996, 50, 19–25.
- Veronese, A.; Garatti, M.; Cipriani, A.; Barbui, C. Benzodiazepine use in the real world of psychiatric practice: Low-dose, long-term drug taking and low rates of treatment discontinuation. Eur. J. Clin. Pharmacol. 2007, 63, 867–873.
Canada:
A ten-year follow-up population-based study from Canada found that despite increased awareness of, and warnings regarding, risks associated with long-term use of benzodiazepines, rates of potentially inappropriate prescribing had changed very little over the period 1996–2006, with 8.4% of subjects using benzodiazepines and 3.5% doing so long-term [1].
A comparison study of benzodiazepine use in Canada and Australia, in which dispensing data was interrogated, found that usage in Canada was over twice that of Australia with a larger number of different drugs being used in Canada and a preference for longer-acting agents in Australia [2].
- Cunningham, C.M.; Hanley, G.E.; Morgan, S. Patterns in the use of benzodiazepines in British Columbia: Examining the impact of increasing research and guideline cautions against long-term use. Health Policy 2010, 97, 122–129.
- Smith, A.J.; Sketris, I.; Cooke, C.; Gardner, D.; Kisely, S.; Tett, S.E. A comparison of benzodiazepine and related drug use in Nova Scotia and Australia. Can. J. Psychiatry 2008, 53, 545–552.
Japan:
In Japan, a large cross-sectional review of psychotropic prescriptions in circa 800 patients with neurotic disorders found that the proportion of subjects being prescribed benzodiazepines for anxiolysis without antidepressants increased with age [1].
Statistics show that Japan has the highest consumption rate in the world. However, benzodiazepines are not included at medical school training for doctors who are largely ignorant on the subject. They prescribe excess amounts, over prolonged periods and poly-prescribe, which is resulting in grave suffering for many unsuspecting victims with absolutely no specialized facilities available to help them.
- Uchida, H.; Suzuki, T.; Mamo, D.C.; Mulsant, B.H.; Kikuchi, T.; Takeuchi, H.; Tomita, M.; Watanabe, K.; Yagi, G. Benzodiazepine and antidepressant use in elderly patients with anxiety disorders: A survey of 796 outpatients in Japan. J. Anxiety Disord. 2009, 23, 477–481.
Thailand:
In Thailand, 45% of GPs surveyed admitted that their prescription of benzodiazepines in the previous year had been excessive: “Practitioners agreed that prescribing should be less than one week (80%); or from 1 week to 1 month (47%); or 1 to 4 months (16%); or 4 to 6 months (5%) or more than 6 months (2%). Twenty-five general practitioners (45%) accepted that they used benzodiazepines excessively in the past year [1].”
A survey of community hospitals in a rural area of Thailand demonstrated that 15% of all adult outpatients received benzodiazepines. These results seem to agree with a previous questionnaire survey among Thai GPs, which found that approximately 50% of them prescribed BZDs for more than 25% of their patients [1].
- Srisurapanont, M.; Garner, P.; Critchley, J.; Wongpakaran, N. Benzodiazepine prescribing behaviour and attitudes: A survey among general practitioners practicing in Northern Thailand. BMC Fam. Pract. 2005, doi:10.1186/1471-2296-6-27.
Brazil:
A cross-sectional study of prescriptions in 3,368 patients visiting a primary health unit in Brazil also showed that 20.6% of prescriptions included BZDs [1]
Although many developing countries allow BZDs to be sold over-the-counter in pharmacies, a literature review of BZD use in Brazil found that the vast majority of BZD consumption was due to medical prescription [2].
- Horta BL, de Lima MS, Faleiros JJ, Weiderpass E, Horta RL: Benzodiazepines: prescription study in a primary health care unit. Revista da Associacao Medica Brasileira. 1994, 40: 262-264.
- Kapczinski F, Amaral OB, Madruga M, Quevedo J, Busnello JV, de Lima MS: Use and misuse of benzodiazepines in Brazil: a review. Subst Use Misuse. 2001, 36: 1053-1069. 10.1081/JA-100104489.
Lebanon:
A recent community survey in Lebanon found that 9.6% (N = 1000) of the population had taken BZD in the previous month [1].
- Naja WJ, Pelissolo A, Haddad RS, Baddoura R, Baddoura C: A general population survey on patterns of benzodiazepine use and dependence in Lebanon. Acta Psychiatr Scand. 2000, 102: 429-431. 10.1034/j.1600-0447.2000.102006429.x.
These trends reflect an ever growing worldwide pandemic, which is having devastating consequences on humanity and society.
To submit more statistics from your particular country or location, please CONTACT US with the information and source.
