The pharmaceutical industry has a long history of romanticizing language. When the word ‘withdrawal’ was thought to evoke negative feelings in relation to psychiatric drugs, the term ‘discontinuation syndrome’ was euphemistically substituted to lower any apprehensions in patients about taking them.
When Valium got a bad rap under the label ‘tranquilizer,’ the term ‘anxiolytics’ was introduced to describe a newer crop of benzodiazepine tranquilizers—Xanax, Ativan, Klonopin, etc—that were more potent but carried smaller dosage labels, deceiving patients into thinking that they were taking a minimal amount when they were actually taking a dose as much as 20 times more potent than an equivalent dose of Valium (1mg of clonazepam [Klonopin] for example, is equivalent to approximately 20mg of diazepam [Valium]).
Not long after Valium’s “bad rap,” the pharmaceutical industry coined the term ‘anxiolytics,’ most likely to distance their new benzodiazepine drugs (Xanax, Ativan, etc.) from the term ‘tranquilizer’ that was associated with Valium. These new benzodiazepines were also promoted and marketed as “non-addicting benzodiazepines”.
Perhaps as an extension of this deceptive marketing—or just because of basic miseducation, misinformation and/or misunderstanding—patients were, and still are, also often reassured (or falsely think on their own) that they are on a “small dose” or a “low dose”. This serves to provide the patient taking the benzodiazepine a false sense of security that taking the benzodiazepine regularly and/or long-term is somehow “safer” because the dose is “small” or “low”. The deceptive marketing has been effective. Unfortunately, this is just more propagation of misinformation and is simply not true.
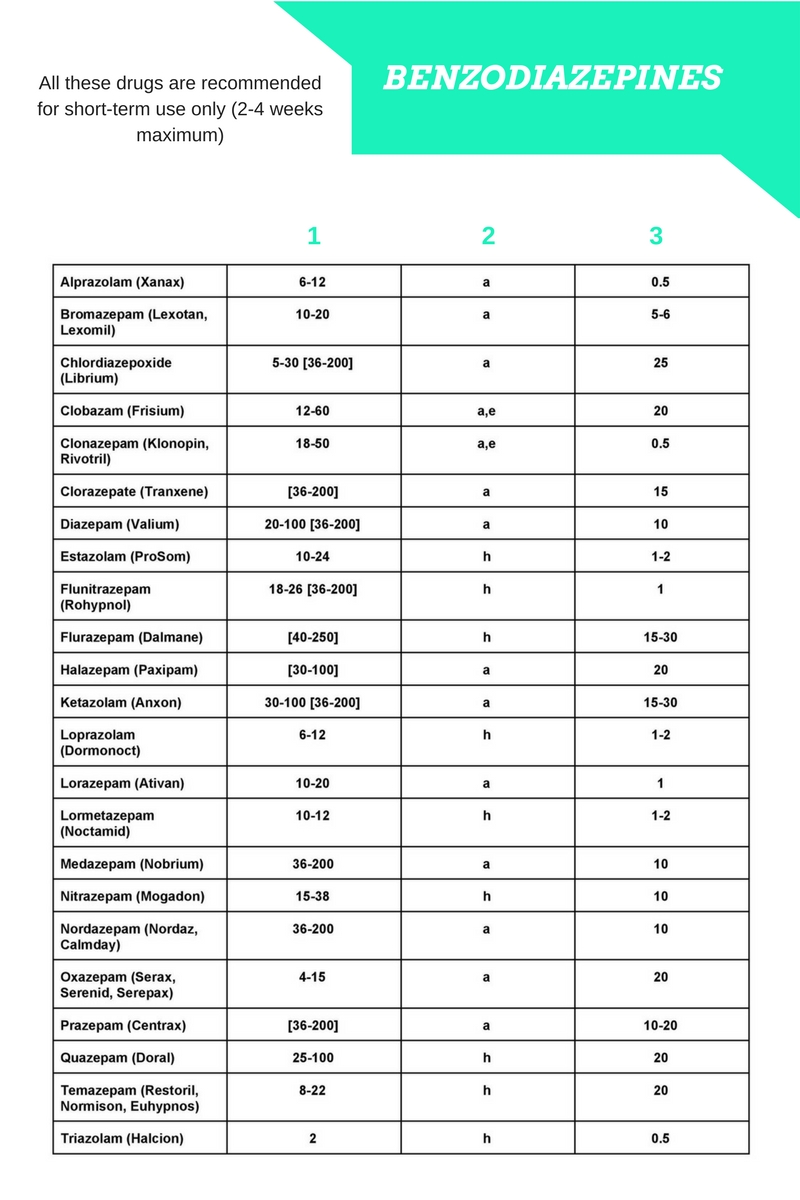
Why is this misinformation occurring? One reason might be that doctors and drug companies have been slow to recognize or differentiate the differences between the many benzodiazepines, both in rates of elimination and in relative potency:
Rates of elimination:
There is considerable individual variation in how people react to benzodiazepines. There are also vulnerable populations (e.g., the elderly) who have reduced metabolism of the benzodiazepines, making them especially susceptible to the sedative effects of the drugs (causing falls and fractures, mental confusion, cognitive impairment, etc.). In addition, there are subtle differences in the pharmacological profiles of the different benzodiazepines, and the equivalences do not always “work” at higher doses (e.g., in clinical experience, diazepam is rather more sedative than lorazepam which is more anxiolytic) when switching between the drugs. People also have variations in the speed at which they metabolize drugs (e.g., fast-metabolizers, slow-metabolizers), but on the whole the equivalences apply generally—except possibly in the case of benzodiazepines which have active metabolites such as diazepam where the half-lives of these can vary from 36–200 hours.
Relative potency:

The three most potent benzodiazepines (or ‘anxiolytics’) are alprazolam (Xanax), clonazepam (Klonopin) and lorazepam (Ativan) which are 10–20 times (lorazepam is 10x more potent; clonazepam and alprazolam are 20x more potent) more potent than diazepam. This difference is often disregarded and the drugs prescribed in excessive dosage because the prescriber is unaware of the equivalent dosages of the benzodiazepines.
So while, say, 0.5mg of Xanax (alprazolam) sounds like a “small dose” or “low dose,” compared to someone taking 10mg of Valium (diazepam), it is not; they are, in fact, equivalent. Someone taking 4mg of clonazepam (Klonopin), which is the maximum recommended dosage for panic disorder, may have no idea that they are being prescribed the equivalent of 80mg of Valium! Four certainly sounds “small” compared to eighty; in reality, they are essentially the same thing (or equivalent). And while, for some, 0.5mg of Xanax (alprazolam) might be efficiently metabolized without notable effects, for others it may not be, causing adverse effects.
Anecdotally, within the benzodiazepine and Z-drug withdrawal support communities, there are numerous reports of individuals taking a so-called prescribed “small dose” or “low dose” (comparatively to other individuals’ larger equivalent doses) who become not only physiologically dependent to those doses (typically when taking them for longer than 2-4 weeks) but who also report withdrawal symptoms and syndromes that are just as severe, distressing and long-lasting as the individuals taking prescribed larger-dose equivalents.
Taking all of this information we know into consideration, the only logical evidence-based conclusion one can arrive at is that there is no such thing as a “small dose” or “low dose” of benzodiazepine. More research into these drugs is desperately needed to make further conclusions.